Initial observation for regression of infantile hemangiomas (IHs) is the current gold standard for treing infantile hemangiomas (IHs). This may be done throughout infancy and youth, with or without pharmacological care with beta-blocker drugs. This treatment plan is effective in virtually totally curing around fifty percent of the lesions. However, the remaining fifty percent of the lesions, particularly established focal IHs of the lip, nose, eyelids, forehead, cheek, and scalp, either do not regress completely with this regimen or do so leaving a deformity; among these lesions, early surgical management may result in a superior aesthetic and functional outcome.
The goal of this study is to identify some localized IH lesions in the head and neck that are likely not going to totally disappear with medical care and that are suitable for a single-stage surgical excision.
In this case series, the senior author analyzed the medical records of babies and children who had presented themselves to a tertiary care vascular abnormalities clinic for the treatment of IHs. For the purpose of this presentation, representative specimens of focal IHs of the lips, nose, eyelids, face, and glabella that demonstrate the influence of tissue expansion have been chosen for display. An expert opinion is presented, which is based on the senior surgeon’s more than 20 years of expertise, during which he treated more than 2000 patients who had focal IH. Additionally, long-term clinical follow-up is included.
elimination of the inflammatory hyperplasia while simultaneously restoring the cosmetic shape and function of the face.
The authors provide five case studies of patients who had effective surgical treatment for localized inflammatory hyperplasia (IH) of the lip, nose, eyelid, cheek, and glabella. The patients all exhibited the tissue expander effect. The ages of the five individuals who were found to have these lesions varied from three months to five years, and all of the patients were female. Before having surgery, one of these patients had an incomplete response to therapy with beta-blockers, while the other patient had an incomplete response to treatment with steroids. In each of these five instances, the tissue expander effect of a localised inflammatory hyperplasia on nearby, unaffected tissue made it easier to remove the lesion and perform primary closure without causing any deformation of the anatomical components. It was showed that the cosmesis may be enhanced while the function remained either same or better.
In babies diagnosed with certain focal infantile hemangiomas, clinicians should strongly consider early surgical surgery as an alternative to protracted observation or medicinal therapy. Although the psychological advantage of early excision of these disfiguring lesions has not been documented, doctors and the relatives of patients report that it is subjectively obvious. Furthermore, the costs and uncertain long-term sequelae of beta-blocker medication, which is the current standard of therapy for IHs together with surveillance for regression, have not yet been quantified but will receive greater salience in the present medical environment. This is because beta-blocker medication is the only treatment that has been shown to be effective against IHs.
The most frequent kind of tumor seen in infants is called an infantile hemangioma (IH). Girls are more likely to be impacted than boys, and head and neck trauma accounts for 65 percent of all traumatic brain injuries.1,2 Additionally, babies with fairer complexion are more likely to be affected with infantile hemangiomas. It has been shown that locations of embryologic fusion are more likely to produce facial IHs than other places.3 Infantile hemangiomas may be either focal or segmental, with the latter kind being more likely to be linked with the PHACES syndrome (posterior fossa brain malformations, large segmental hemangiomas, vascular anomalies, cardiac/heart anomalies, ear/eye/endocrine abnormalities, sternal cleft/supraumbilical raphe). Lesions of the airway may also be observed in either a focal or segmental distribution, and they are especially related with IHs that occur in the V3 segment.
The clinical history of infantile hemangiomas is characterized by early fast proliferation in the first few months of life, followed by a period of quiescence, and then a period of slower spontaneous involution starting at roughly 9 months of age. This pattern of progression is seen in all infantile hemangiomas. The majority of lesions heal on their own, while some react well to medical treatments on their own and do not call for surgical intervention. Other lesions may only partly involute on their own or with the help of medical therapy. In these cases, surgery will be necessary to correct any aesthetic or functional deformity that is still present.
This article aims to underline that surgical therapy should play a key role in the management of certain lesions. This is one of the objectives or goals of this article.4 These lesions include those that affect vital functions (breathing, eating, and vision), focal lesions that are resistant to medical therapy, ulcerated and bleeding lesions, and select large, cosmetically deforming lesions, such as those involving the lips, nose, eyelid, cheek, and glabella, that are likely to respond poorly to -blocker therapy (for example, propranolol therapy). Delaying surgical surgery in favor of extended medical care for these individuals is often not beneficial and may have a detrimental impact on the psychological well-being of a kid as well as the well-being of his or her family.
Because of this, surgery need to be regarded as the main therapeutic option for focal IHs of the lips, nose, eyelids, forehead, glabella, cheeks, and scalp that have not responded well to therapy with beta-blockers. At least half of the focal IHs that are treated with propranolol throughout infancy and youth may, at some point in the future, need surgical or laser therapy due to either partial involution while under medicinal care or secondary abnormalities.5,6
When an IH is in its enlarged condition, just before to the process of involution, there is often superfluous skin and tissue that might be of assistance to a surgeon in the process of eliminating the lesion. In these situations, total or almost complete removal is possible without causing any deformation to the anatomical location. During the process of involution, or as a consequence of just a partial response to medical care, this impact is lost. Because of this, it is advantageous to treat these big focal lesions surgically at a period when it is still early in the process.
As an example, we choose to focus on these five exemplary scenarios. We chose one patient with an IH as an example from each of the following locations: the lip, the nose, the eyelid, the cheek, and the glabella. The forehead and the scalp are other places that illustrate the tissue expansion effect; however, due to the restrictions of the figures in this study, we do not offer instances of those sites. These constraints prevented us from showing examples of the forehead and the scalp. The patients who were chosen were babies and children who had focal IHs. Their lesions had been surgically excised, and their defects had been healed with mostly positive aesthetic and functional effects. At a tertiary care referral facility, the same primary surgeons, M.W. and T.M.O., provided treatment for each of the patients. In this context, the elimination of the IH while simultaneously restoring the aesthetic shape and function of the face is considered to be successful therapy. The institutional review board of Lenox Hill Hospital at Northwell Health System (formerly known as Northshore LIJ Health System) gave its clearance to proceed with this research project. All of the patients’ parents or legal guardians provided their written approval after being informed.
At the time of surgery, the ages of the five patients who were included in this case series varied from three months to five years, and three of them were female. Each patient was given therapy with beta-blockers, although the patients only showed a partial reaction to the medication.
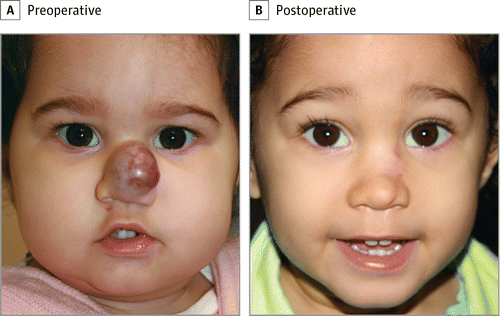
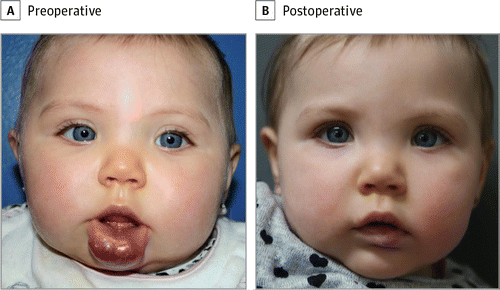
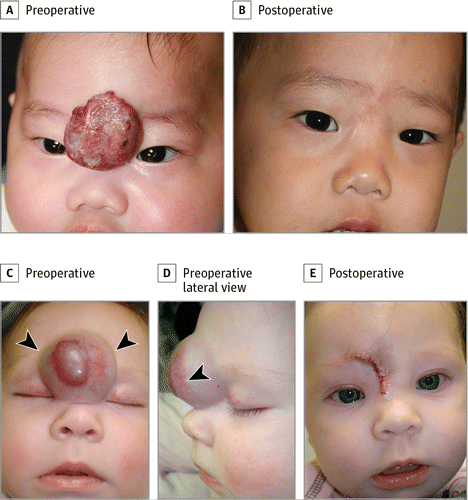
The illustration in Figure 1A shows an extensive IH that affects more than 65% of the lower lip. The medical treatment did not cause this lesion to shrink, rather instead it continued to expand. Before having surgery at the age of 5.5 months, the kid was given propranolol for a period of four months as part of the therapy process. The IH itself induced significant enlargement of the lip, which made it possible to remove more than 95% of the IH and achieve primary closure without the development of microstomia as a consequence. Figure 1B illustrates the minute amount of residual lesion that persisted after the first treatment with pulsed dye laser and went on to be eliminated.
A, the condition affected more than 65 percent of the lower lip. The inflammation generated a significant increase in tissue growth. Without performing microstomia, almost 95% of the hemangioma was successfully eliminated. B, A treatment with a pulsed-dye laser was performed on the erythema that was still present.
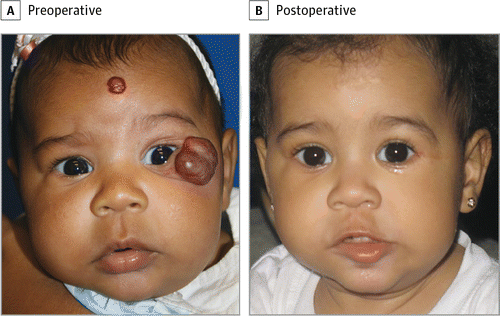
Figure 2 displays a young girl who was treated medically with propranolol for an IH of the lower eyelid but did not see any improvement in her condition. Because of the tissue expansion effect caused by the localized inflammatory hyperplasia, an increased quantity of resection was possible in comparison to the typical amount. It was possible to execute a wedge excision without causing considerable eyelid shortening or ectropion, which led to a successful outcome in terms of the patient’s aesthetic appearance. When therapy begins early, it is possible to reverse the effects of astigmatism and prevent any irreversible vision loss that may have been caused by the pressure of the mass. Eyelid lesions that cause unilateral astigmatism should ideally be removed before to the age of 9 months, if at all possible.
IH exhibited (A) before and (B) after surgical removal of the lesion. Due to the tissue expander effect, total removal was possible without the need for ectropion.
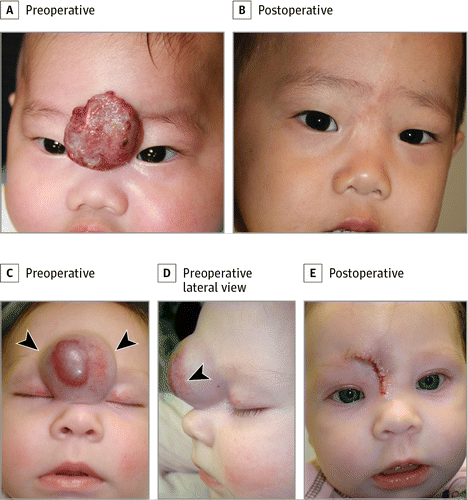
Figure 3A and 3B depict a patient who has a substantial amount of ulceration along with a big focal infantile hemangioma of the glabella. This patient’s lesion did not react to the medicinal care that was being administered, and it was causing substantial discomfort as well as bleeding. Before undergoing excision at the age of 6 months, the kid had steroid treatment for a period of one month in an institution located outside of the home. On the other hand, there was no discernible growth of the tissue that was located next to the mass in the glabellar area in this patient. After the bulk was removed, there was no longer any tissue expander effect, which led to the inevitable medialization of the brows, providing an appearance similar to that of a “unibrow.”
A and B, The lack of a tissue expander effect resulted in the medialization of the eyebrows, sometimes known as the “unibrow” effect. The arrowheads in C-E illustrate the impact of the tissue expander on the patient’s body. The bulk was proven to have been removed during the procedure itself, and there was no medialization of the eyebrows at any point throughout the process.
Figure 3C-E depicts a youngster who, like the previous patient, had an IH of the glabella. This child’s lesion, in contrast to the patient whose images are shown in Figure 3A and B, generated a large tissue expansion impact on the surrounding tissue in the glabella that was not affected by the mass. After the lesion was removed, the enlarged tissue could be reapproximated and closed without any strain at all.
A youngster with an IH of the nasal dorsum, tip, alae, and sidewalls that did not respond fully to a course of steroid therapy is shown in figure 4. The injury caused the nearby, undamaged tissue to expand, resulting in tissue expansion. In order to successfully remove the IH, a modified subunit method was used, and primary closure was accomplished with the assistance of the tissue expansion effect.7 The patient’s attractiveness improved after surgery, and she also found relief from the nasal blockage that she had been suffering from before.
A, take note of the enlargement of the tissue. B, The image of the youngster was taken roughly one year after the IH was surgically removed, taking advantage of the tissue growth at that time.
The impact of a large focused IH on the cheek tissue of a young girl is seen in Figure 5. This results in the tissue expanding. She was given a treatment that consisted of a single-stage surgical excision, which only required the removal of the affected skin and subcutaneous tissue. The IH reached all the way down to the deep fascial layer, which covered the muscles that control face expression. Primary closure was performed without changing the shape of the cheek or causing strain on the neighboring lip, ala, or eyelid. All but a little rim of the cutaneous component of this IH was excised, and the closure was accomplished without any complications.
Several examples of focal IH that were effectively treated by surgical excision are shown here. individuals who have focal IHs of the lips, nose, eyelid, forehead, or glabella and whose lesions have not retreated with -blocker medication during the proliferative period (the first year of life) may benefit from early surgical surgery. This is especially true for individuals who have focal IHs of the lips, nose, eyelid, forehead, or glabella. By selecting for early surgical surgery, these individuals may avoid years of living with a cosmetic and/or functional deformity, as well as months of monitoring and/or therapy with propranolol, if they are treated early. Additionally, they can avoid the possibility of saving years of their lives.
Because of the influence that isolated intrahepatic hemorrhages have on the growth of tissue, it is technically simpler to execute surgical surgery on newborns and young children. The overlaying skin and the subcutaneous tissue are both stretched because the IH is expanding as it grows. Hemangiomas in infants do not spread into the surrounding tissue in any way. Instead, they push the tissues that are around them out of the way and compact a plane of soft tissue around themselves. This tissue plane makes it easier for the surgeon to dissect the tissue, and as long as the surgeon stays in this tissue plane while he or she is dissecting, there will be less loss of blood. By stretching the skin overlaying the wound, primary closure may be achieved without causing excessive skin tension or distorting the anatomy, creating an excellent environment for wound healing in infants. Collagen type II is produced in lower quantities by infants and children less than three years of age compared to older children and adults.8 By taking use of this biological function, fibrosis will be reduced, and the end outcome will be one with greater cosmetic quality.
The multiplication and growth of the hemangioma is what causes the tissue expander effect to take place. This, in turn, causes the overlying skin to expand and displaces the tissue that is close to it. This effect does not appear all of the time, but when it does, it can only be seen when the hemangioma is in its enlarged stage. Because the quantity of inflated skin diminishes as the lesion shrinks, it is eliminated during the late involution phase or after a partial response to propranolol. This is the case for both of these phases. At this point, it may be necessary to keep the skin that is associated with the hemangioma in place in order to accomplish primary closure and avoid distorting the anatomy.
It bears repeating that focused intrahepatic hematomas, in particular those that are treated at a later point in their development cycle and have developed to form a substantial mass, have a tendency to react less favorably to medical therapy. This is something that should not be overlooked.5 In addition to this, a subgroup of patients with localized inflammatory hyperplasia of the lip, nose, eyelids, forehead, face, glabella, or scalp may first appear for therapy after the proliferative phase of the inflammatory hyperplasia has concluded. At this late stage of a focal IH, beta-blocker medication is unlikely to be successful in treating the condition. In situations like these, the lesion may be removed by taking advantage of the tissue expansion effect that the lesion itself has on the normal tissue that is close to it. This allows the lesions to be treated without leaving behind a substantial aesthetic or functional defect. Before deciding whether or not to do surgery, it is important to first examine the kid between the ages of one and five to seven years to determine the extent to which the lesion has disappeared. This monitoring is an option for patients who have not suffered any deformity, anatomical deformation, or functional impairment as a result of their condition. On the other hand, even a lesion that has completely disappeared may still leave behind a mass of fibrofatty tissue or atrophic skin that is aesthetically unappealing in certain parts of the face. This is the case the majority of the time.
In the cases that included the lower lip, excision of the IH was done, and then the lip was closed without leaving a large amount of microstomia. In order to avoid the development of microstomia, it is recommended that a wedge resection of the lower lip never take up more than thirty percent of the area of the lower lip. Lower lip hemangiomas always produce soft tissue expansion, which extends the neighboring lip and makes it possible to remove a greater amount of the lip during surgery. In circumstances like these, we often have to resect up to fifty percent of the lip. If the lesion were to encompass a larger area of the lower lip, a wedge excision may be done. During this procedure, some of the hemangioma would be left behind to enable closure without significantly reducing the lip. Propranolol may be administered to the patient during surgery in the case that the IH is still proliferating at the time of the procedure in order to stop any further proliferation. In many instances, medical treatment is sufficient to eradicate the lesion without causing any substantial disfigurement to the lip’s appearance. Later on in childhood, if there is a tiny amount of residual ichthyosis (IH) or atrophic or scarred skin, it may be addressed with a mild surgical or laser surgery for the purpose of aesthetic improvement.
In the case involving the eyelid, initial wound closure was accomplished without generating ectropion or distorting either the upper or lower eyelid. Because of the influence that the IH’s proliferation had on the enlargement of the tissue, the function of the eyelids and their ability to close were not affected.
In the case of IHs of the cheek, the tissue expander effect will often make it possible for surgical excision of the majority of the cutaneous component of the disease while still allowing for the natural shape of the cheek to be preserved. If surgery is postponed for an extended period of time and the IH partly involutes, this benefit will be lost. In the example that was brought to us, we were able to resect the whole deep component while leaving a tiny rim of cutaneous lesion in order to avoid the cheek from being too shortened. After that, a pulsed dye laser was used to treat this localized portion of the skin.
Patients and their families may avoid having to make many trips to the doctor and being exposed for a longer period of time to a medicine whose long-term effects in newborns and children are still being researched if early surgical intervention is performed. When treating a kid who has IH with beta-blockers, a normal course of medication may run for up to six months. The concept that a kid should take medicine for an extended period of time is met with resistance from many parents. Despite the fact that the cardiovascular safety profile of propranolol medication has been established in a number of studies9,10, there are additional negative effects of propranolol that have not been investigated in children. Research conducted on mice has shown evidence that propranolol may prevent the formation of new memories.11 It has been shown that propranolol prevents the consolidation and reconsolidation of emotional memories in adults who are healthy. This property indicates promise as a potential treatment for people who suffer from posttraumatic stress disorder.12 There are no studies that we are aware of that have been conducted to date that investigate the impact, if any, on memory acquisition among newborns and young children who have been subjected to propranolol medication for the treatment of IHs for a period of six months or more. In addition, one of the most prevalent side effects of propranolol is sleep disruption, which shows that there is a central impact. This finding supports the hypothesis that there is an effect. For these reasons, early surgical surgery is recommended for patients with focal IHs, in whom medical care has been found to be less beneficial than in patients with segmental IHs. Patients with segmental IHs are more likely to benefit from medical management.